Cost-related non-adherence to glaucoma medication in glaucoma patients attending an eye
hospital in Western Nepal
Ravi Dhar Bhandari, Dhangadhi Netralaya Eye Hospital, Dhangadhi, Nepal
Jeewanand Bist, Tilganga Institute of Ophthalmology, Kathmandu, Nepal
Manish Poudel, Tilganga Institute of Ophthalmology, Kathmandu, Nepal
Om Prakash Pant, Dhangadhi Netralaya Eye Hospital, Dhangadhi, Nepal
Bidhya Prasad Pant, Dhangadhi Netralaya Eye Hospital, Dhangadhi, Nepal
Keywords: cost, glaucoma, medication, non-adherence
Abstract
Objective
The objective of this study was to assess the magnitude and factors associated with cost-related
non-adherence (CRNA) to medical glaucoma therapy.
Methods
A cross-sectional hospital based study was conducted at Dhangadhi Netralaya Eye Hospital in
the western Nepal. The study included all consecutive glaucoma patients aged 18 and above and
have been under medical glaucoma therapy for at least six months. A face-to-face interview was
conducted to record the socio-demographic details of the participants and to assess
non-adherence to therapy.
Analysis
The burden of CRNA was assessed by estimating the proportion of CRNA with 95% confidence
interval (CI). The association between dependent variable (CRNA) and independent variables:
age, gender, presenting visual acuity right eye, duration of glaucoma, number of bottles of
glaucoma medicines prescribed, presence of systemic disease(s) and disability were assessed in a
bivariate analysis. A logistic regression was conducted to adjust the confounding variables. A
p-value less than 0.05 was considered significant.
Results
The study included 132 participants; 80 males (60.6%) and 52 females (39.4%). The mean age of
the included participants was 60.1 years (SD ±12.6; range 28 to 82 years). The majority of
included participants had primary open angle glaucoma (37.9%) followed by primary angle
closure glaucoma (22.7%). The mean duration of glaucoma was 4.2 years and the mean duration
of medication was 4 years. CRNA was observed in 14 (10.6%; 95% CI 6.1 -17.5) patients. In a
bivariate analysis, age (p=0.545), gender (p=0.0842), presenting visual acuity (p=0.899),
employment status (p=0.230), and presence of disability (p=0.161) showed statistically
insignificant association with medication non-adherence while number of medicine bottles
prescribed (p<0.001) and duration of glaucoma (p=0.0432) showed statistically significant
association. Similarly, in a logistic regression, gender, number of glaucoma medicines prescribed
and presence of systemic disease(s) showed statistically significant association with CRNA.
Conclusion
The cost-related non-adherence to glaucoma medical therapy was present in 1 in 10 individuals
with glaucoma. Gender, presence of systemic disease(s) or co-morbidity and number of
glaucoma medicines prescribed were significantly associated with cost-related non-adherences.
Key messages
What is already known on this topic?
The medical management of glaucoma involves a long term medication. Therefore, a good
adherence to the prescribed therapy is important. However, adherence to glaucoma medication is
often poor.
What this study adds
Cost is an important barrier to glaucoma medication. Gender, presence of systemic disease(s) or
co-morbidity and number of glaucoma medicines prescribed are significantly associated with
cost-related non-adherence to glaucoma medical management
How this study might affect research, practice or policy
This study provides significant implications both at clinical and policy levels. Understanding the
magnitude and factors associated with non-adherence to medication are important to formulate
policies to reduce the non-adherence rates.
Introduction
Glaucoma is a leading cause of irreversible vision impairment globally.1 The medical
management of glaucoma involves a long term medication. A good adherence to the prescribed
therapy is necessary; however, unfortunately, adherence to therapy is often poor. Among the
many causes of medication non-adherences such as, forgetfulness, difficulty with drop
administration, shortages of medicines particularly in the rural areas and complexity of
medication regimen, cost has also been an important determinant for non-adherence.2–7 In one of
the recent reviews on glaucoma medication adherences, Moore et al2 reported higher medication
costs, a significant factor for medication non-adherence. Similarly, in a recent study in North
India, nearly one-quarter of medication non-adherences were because of cost issues.3
Cost-related non-adherence is a condition when a patient does not take their medications as
prescribed because of financial an issues. They may lower the dosage, skip taking medications,
follow-up late, revert to alternative medications or borrow money/take a loan to overcome the
cost of therapy. Although nearly 2%8 of Nepalese population is found to have glaucoma and a
substantial number is expected to have the disease in the coming years, there have not been robust
evidence on the cost and cost-related adherence to glaucoma therapy. Cost has been an important barrier
in undertaking therapy, more particularly in the developing countries.9–11 Understanding the burden and
risk factors for cost-related glaucoma medication non-adherence are therefore important, particularly to
reduce glaucoma related visual disability and also for formulating policies to minimize non-adherences.
In this regard, this study was aimed to assess the magnitude of CRNA and associated factors for
non-adherence.
Materials and Methods
This was a cross-sectional hospital based study conducted at Dhangadhi Netralaya Eye Hospital
in the western part of Nepal. The study was approved by the Ethical committee of Nepal Health
Research Council (protocol ref no.: 54). Informed and written consents were obtained from all
participants before recruiting them to the study.
The study included all consecutive glaucoma patients attending the hospital from 01 October
2023 to 31 March 2024 and have been under medical glaucoma therapy for at least six months.
Only patients aged 18 and above were included in the study. All patients were seen by a
glaucoma specialist at the hospital and a diagnosis was made based on clinical examinations.
Visual acuity in the included participants was assessed using a Snellen chart and the recorded
Snellen acuity was converted to decimal acuity. Participants with presenting visual acuity less
than 6/12 in the better eye were categorized as visually impaired while those with <3/60 in the
better eye were categorized as blind.
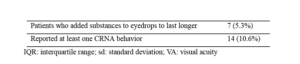
A face-to-face interview was conducted to record the socio-demographic details of the
participants and to assess non-adherence to therapy. CRNA was considered if, in the last six
months, the patient: a) reduced, or skipped medication dosage to save money b) delayed filling
prescription because of cost issues, c) reverted to alternative therapies because of cost, or d)
added anything to the eye drops to last longer.
Data analysis was conducted in R software (version 4.3.3).12 First, the data were entered in
MS-Excel where the data were cleaned and coded. Next, the excel sheet was imported to R
where analysis was performed. Univariate analysis was computed using percentage for
categorical variables while mean ± SD were calculated for numerical variables. The burden of
CRNA was assessed by estimating the proportion of CRNA with 95% confidence interval (CI).
A bivariate analysis was conducted to assess the association between dependent variable
(CRNA) and independent variables: age, gender, presenting visual acuity right eye, duration of
glaucoma, number of bottles of glaucoma medicines prescribed, presence of systemic disease(s)
and disability. A chi-square test was used for categorical variables while for a numerical
independent variable, a Mann-Whitney U test or t-test was used depending on the distribution of
the data. Further, to adjust for the cofounding variables, a logistic regression analysis was
performed using the Enter method and odds ratio were estimated. A p-value less than 0.05 was
considered significant.
Results
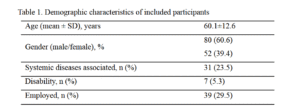
The study included 132 participants; 80 males (60.6%) and 52 females (39.4%). The mean age of
the included participants was 60.1 years (SD ±12.6; range 28 to 82 years). The demographic
characteristics of included participants is presented in
Table 1.
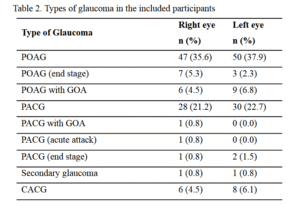
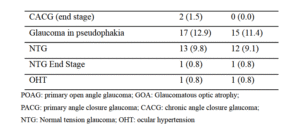
The study included patients with different types of glaucoma who were under topical glaucoma
medication for more than six months. The majority of included participants had primary open
angle glaucoma (37.9%) followed by primary angle closure glaucoma (22.7%). The details of the
type of glaucoma in the included participants are presented in Table 2. The mean duration of
glaucoma was 4.2 years and the mean duration of medication was 4 years. Single glaucoma
medicine bottle was prescribed in 83 patients (62.9%) and multiple bottles in 37.1% patients: 2
bottles in 28.8% and three bottles in 8.3% of included participants.
Table 2. Types of glaucoma in the included participants
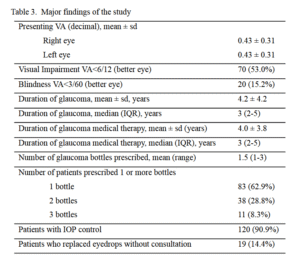
The mean presenting decimal visual acuity in the included participants was 0.43 ± 0.31 (6/14
snellen equivalent) in both eyes. Visual impairment and blindness was present in 53.0% and
15.2% of the included participants. At least one CRNA behavior was observed in 14 (10.6%;
95% CI 6.1 -17.5) patients. The major findings of the study are presented in Table 3.
Table 3. Major findings of the study
In a Mann-Whitney U test, age and presenting visual acuity showed statistically insignificant
association with medication non-adherence (age p=0.545, and presenting acuity p=0.899) while
number of medicine bottles prescribed (p<0.001) and duration of glaucoma (p=0.0432) showed
statistically significant association. Similarly, association of non-adherence with gender was
assessed using a Chi-square test while associated systemic disease(s), presence of disability and
employment status was assessed using Fisher’s exact test. Gender (χ2=2.981, p=0.0842),
employment status (OR=2.72, p=0.230), and presence of disability (OR=0.27, p=0.161) were not
statistically significant while presence of systemic disease(s) (OR=0.89, p<0.001) showed
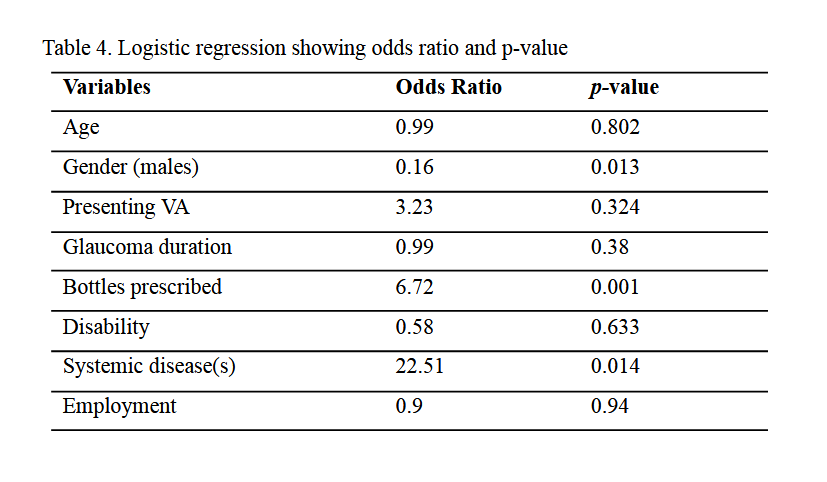
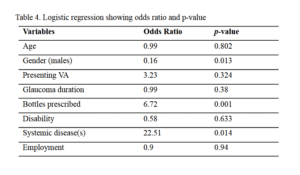
statistically significant association with CRNA. Further, when confounding variables were
adjusted in a logistic regression, gender, number of glaucoma medicines prescribed and presence
of systemic disease(s) showed statistically significant association with CRNA. Presence of
systemic disease(s) increased the risk of non-adherence by nearly 22 times while prescribing
more than one medicine for glaucoma increased the risk by nearly 7 folds. The results of logistic
regression are presented in Table 4.
Table 4.
Discussion
The present study was conducted to assess CRNA to glaucoma medical therapy. In a consecutive
sample of 132 patients with different types of glaucoma, CRNA was observed in 10.6% of
participants. The patients showing non-adherence to medication were found to skip, reduce or
add something to the drops to last longer or save money. The study also determined the factors
associated with CRNA. Gender, glaucoma multi-medication, and presence of systemic diseases
were factors significantly associated with glaucoma medication non-adherence.
Cost is an important barrier to glaucoma therapy; however, there have not been many studies that
have assessed non-adherence because of cost issues. Buys et al6 conducted a study in a Canadian
population and estimated 25.8% CRNA in glaucoma patients aged 25-64 years and 7.1% in
people aged above 65 years; a cumulative 15.5% non-adherence was observed when all age
groups were considered. Interestingly, they found a greater non-adherence in younger patients
compared to the elderly. Unlike in Buys et al6 study, we did not find a significant association
between age and non-adherence. It may be because in Buys et al study, majority of elderly
people used insurance to purchase medicines while most of the young patients did not have the
insurance.
Similarly, Gupta et al13 compared cost related issues in patients with glaucoma and without
glaucoma. They found that patients with glaucoma faced significantly more cost related
challenges than those without glaucoma. In their study, CRNA was reported in 32% of patients
while another 20% asked their doctor to prescribe cheaper drugs. The proportion of CRNA
reported by Gupta et al13 is much higher than that reported in our study.
In another study conducted in the United States, Blumberg et al5 reviewed the Medicare Current
Beneficiary Survey data from 2004 to 2009 to assess the trends in cost reduction and cost saving
behaviors of Medicare beneficiaries with glaucoma before and after the administration of
Medicare prescription drug benefit. They reported 21% CRNA in 2004 which reduced to 7.6% in
2009 after the implementation of the Medicare prescription drug benefit. They also analysed the
independent risk factors associated with CRNA and found that the associated risk factors were
lower income, younger age, self-reported visual disability, and limitations in activities of daily
living. Further, individuals without any form of prescription drug coverage or with greater
co-morbidities were more likely to show CRNA behavior. In our study, although we did not
study the effect of income on CRNA; our results are consistent with Blumberg et al5 study which
showed presence of co-morbidity as a significant risk factor for CRNA. Presence of systemic
disease(s) increased the risk of non-adherence by 22 folds in our study. This appreciably high
non-adherence rate in co-morbid patients in our sample may be because of high costs incurred in
purchasing medicines for multiple diseases. Most importantly, no patients in our sample used
insurance to purchase medicines. Also, literature suggests that individuals with multi-morbidity
usually experience increased out-of-the pocket health care expenses and are more prone to cost
related non-adherences.14–17
Another important factor for medication non-adherence in our study was multi-medication.
Prescribing complex multi-drug regimens is common in glaucoma medical management,
particularly, when the intraocular pressure cannot be controlled with a single medication.18
However, added number of drugs is found to significantly decrease medication adherence. These
findings are consistent with a recent comprehensive systematic review which reported complex
eye drop regimens as one of the important factors for non-adherences.19
Our present study has several strengths. First, we were able to prospectively assess the burden of
CRNA in a Nepalese cohort with glaucoma. Reports on CRNA in glaucoma patients in Nepalese
population are scarce and therefore, this study provides important baseline data for further large
population based studies. Although the results of our study are important and interesting, there
are certain limitations of the study. Most importantly, the present study was limited by the
number of participants included in the study. A larger sample size would have produced more
robust results. Because glaucoma is not a very common disease, it is always difficult to include a
large number of participants in a prospective study. However, the authors recommend that more
studies in different geographic locations of the country with larger sample sizes be conducted for
the generalizability of the findings.
Conclusion
Adherence to medication therapy is an important aspect of glaucoma management. In
low-and-middle-income countries non adherence to medication due to higher cost of medication
plays a crucial role. The results of our study showed that cost-related non-adherence was present
in 1 in 10 individuals with glaucoma. Gender, presence of systemic disease(s) or co-morbidity
and number of glaucoma medicines prescribed were significantly associated with cost-related
non-adherences.
References
1. Flaxman SR, Bourne RRA, Resnikoff S, Ackland P, Braithwaite T, Cicinelli M V., et al.
Global causes of blindness and distance vision impairment 1990-2020: a systematic
review and meta-analysis. Lancet Glob Heal [Internet]. 2017 Dec 1 [cited 2022 Apr
10];5(12):e1221–34. Available from: https://pubmed.ncbi.nlm.nih.gov/29032195/
2. Moore SG, Richter G, Modjtahedi BS. Factors Affecting Glaucoma Medication
Adherence and Interventions to Improve Adherence: A Narrative Review. Ophthalmol
Ther [Internet]. 2023 Dec 1 [cited 2025 Apr 25];12(6):2863–80. Available from:
https://link.springer.com/article/10.1007/s40123-023-00797-8
3. Singh K, Singh A, Jain D, Verma V. Factors affecting adherence to glaucoma medication:
Patient perspective from North India. Indian J Ophthalmol [Internet]. 2024 Mar 15 [cited
2025 Apr 25];72(3):391–6. Available from:
https://journals.lww.com/ijo/fulltext/2024/72030/factors_affecting_adherence_to_glaucom
a.18.aspx
4. Negese Kebede B, Mohammed Seid S, Kefyalew B, Gesese E. Glaucoma medication
non-adherence rate and associated barriers among glaucoma patients in Hawassa,
Ethiopia. BMC Ophthalmol [Internet]. 2024 Dec 1 [cited 2025 Apr 25];24(1):490.
Available from:
https://bmcophthalmol.biomedcentral.com/articles/10.1186/s12886-024-03750-w
5. Blumberg DM, Prager AJ, Liebmann JM, Cioffi GA, De Moraes CG. Cost-Related
medication nonadherence and cost-saving behaviors among patients with glaucoma before
and after the implementation of medicare part D. JAMA Ophthalmol. 2015 Sep
1;133(9):985–96.
6. Buys YM, Kagan D, Jin YP, Trope GE. Cost-related nonadherence with glaucoma
medications in Ontario. Can J Ophthalmol [Internet]. 2021 Dec 1 [cited 2022 Apr
9];56(6):379–84. Available from: https://pubmed.ncbi.nlm.nih.gov/33548175/
7. Spencer SKR, Shulruf B, McPherson ZE, Zhang H, Lee MB, Francis IC, et al. Factors
Affecting Adherence to Topical Glaucoma Therapy: A Quantitative and Qualitative Pilot
Study Analysis in Sydney, Australia. Ophthalmol Glaucoma. 2019 Mar 1;2(2):86–93.
8. Thapa SS, Paudyal I, Khanal S, Twyana SN, Paudyal G, Gurung R, et al. A
population-based survey of the prevalence and types of glaucoma in Nepal: the Bhaktapur
Glaucoma Study. Ophthalmology [Internet]. 2012 Apr [cited 2022 Apr
10];119(4):759–64. Available from: https://pubmed.ncbi.nlm.nih.gov/22305097/
9. Adio AO, Onua AA. Economic burden of glaucoma in Rivers State, Nigeria. Clin
Ophthalmol [Internet]. 2012 Dec 4 [cited 2025 Mar 26];6(1):2023. Available from:
https://pmc.ncbi.nlm.nih.gov/articles/PMC3526906/
10. Musa I, Bansal S, Kaleem MA. Barriers to Care in the Treatment of Glaucoma:
Socioeconomic Elements That Impact the Diagnosis, Treatment, and Outcomes in
Glaucoma Patients. Curr Ophthalmol Rep [Internet]. 2022 Sep 1 [cited 2025 Mar
26];10(3):85–90. Available from:
https://link.springer.com/article/10.1007/s40135-022-00292-6
11. Murdoch I, Smith AF, Baker H, Shilio B, Dhalla K. The cost and quality of life impact of
glaucoma in Tanzania: An observational study. PLoS One [Internet]. 2020 Jun 1 [cited
2025 Mar 26];15(6). Available from: https://pubmed.ncbi.nlm.nih.gov/32479506/
12. R Core Team. R: A Language and Environment for Statistical Computing [Internet].
Vienna, Austria: R Foundation for Statistical Computing; 2021. Available from:
https://www.r-project.org/
13. Gupta D, Ehrlich JR, Newman-Casey PA, Stagg B. Cost-Related Medication
Nonadherence in a Nationally Representative US Population with Self-Reported
Glaucoma. Ophthalmol Glaucoma. 2021 Mar 1;4(2):126–30.
14. Larkin J, Foley L, Timmons S, Hickey T, Clyne B, Harrington P, et al. How do people
with multimorbidity prioritise healthcare when faced with tighter financial constraints? A
national survey with a choice experiment component. BMC Prim Care [Internet]. 2025
Feb 27 [cited 2025 Mar 26];26(1):57. Available from:
https://pmc.ncbi.nlm.nih.gov/articles/PMC11866811/
15. Larkin J, Walsh B, Moriarty F, Clyne B, Harrington P, Smith SM. What is the impact of
multimorbidity on out-of-pocket healthcare expenditure among community-dwelling older
adults in Ireland? A cross-sectional study. BMJ Open. 2022 Sep 1;12(9).
16. Anindya K, Ng N, Atun R, Marthias T, Zhao Y, McPake B, et al. Effect of multimorbidity
on utilisation and out-of-pocket expenditure in Indonesia: quantile regression analysis.
BMC Health Serv Res. 2021 Dec 1;21(1).
17. McRae I, Yen L, Jeon YH, Herath PM, Essue B. Multimorbidity is associated with higher
out-of-pocket spending: A study of older Australians with multiple chronic conditions.
Aust J Prim Health. 2013;19(2):144–9.
18. Khouri AS, Realini T, Fechtner RD. Use of fixed-dose combination drugs for the
treatment of glaucoma. Drugs and Aging [Internet]. 2007 Aug 31 [cited 2025 Apr
25];24(12):1007–16. Available from:
https://link.springer.com/article/10.2165/00002512-200724120-00004
19. Bott D, Subramanian A, Edgar D, Lawrenson JG, Campbell P. Barriers and enablers to
medication adherence in glaucoma: A systematic review of modifiable factors using the
Theoretical Domains Framework. Ophthalmic Physiol Opt [Internet]. 2024 Jan 1 [cited
2025 Apr 25];44(1):96–114. Available from: https://pubmed.ncbi.nlm.nih.gov/37985237/
